Command the Invisible.
Fast-Track Hands-On Ultrasound Training for Clinicians Ready to Use It at the Bedside.

Learn to Scan, Interpret and Think in Ultrasound.
Live, micro-group classes with real scanning, real-time correction, and faculty at your elbow.
Clinical service since 1975.
Founded 1981 at the University of Texas Southwestern Medical University in 1981.
Academically independent since 1987.
Open Classes
Held in Dallas, Texas. USA


Real anatomy. Hands-On Scanning. 24 Hr Scan Lab. Lifetime Mentoring.
Write your text here...




Write your text here...
Total protocol. Total understanding.
Every stage. Clearly seen.
Systematic scans. Deeper insight.
Clarity. Where it matters.
Hands-On Transvaginal Pelvic Ultrasound
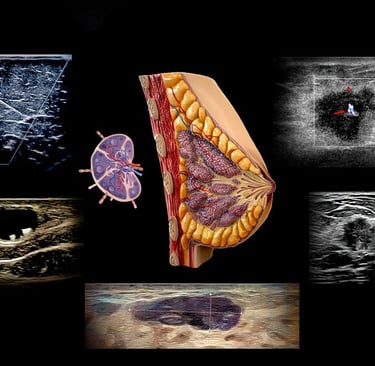
Hands-On Breast Ultrasound
Detect early. Understand fully.
Hands-On Obstetric Ultrasound
Hands-On Cardiac Ultrasound: Echocardiography
Hands-On Vascular Ultrasound:
Total Body
Introduction to Hands-On Ultrasound for Clinicians New to It
Foundation first. Clarity always.
See clearly. Decide faster.
POCUS: Point of Care Bedside Ultrasound
Hands-On Abdominal Ultrasound
Write your text here...
Write your text here...
Write your text here...
Write your text here...





Flow understood. Disease revealed.
Training Clinicians Worldwide Since 1981.
Testimonials reflect individual learning experiences. Growth in skill and confidence develops through guided training, continued practice, and personal commitment.
Contact
972 | 353-3200 USA Central Time
Course Campus:
4300 Wingren Drive
Irving (Las Colinas), Texas 75039
Mail | FedEx Address:
Box 101
Colleyville, TX 76034
Courses & Learning
Hands-On Clinical Courses
Ultrasound Physics
Cardiovascular Hemodynamics
EKG- From Atoms to Arrhythmias
Privacy Policy | Terms of Use. | Disclaimer
We’re committed to accessibility. View our Accessibility Statement.
The most powerful technology in medicine
is the person using it.